
It is 3 AM. Your nipples are cracked. Your baby is rooting, frustrated, and crying. And every piece of advice you have been given feels like it belongs to someone else’s body, someone else’s baby.
You were told breastfeeding would be natural. Instinctive. Beautiful. And here you are, googling in the dark, wondering why your body seems to have missed the memo. I need you to hear something clearly: that feeling is not evidence of failure. That feeling is evidence that no one gave you the whole story.
The position you were most likely taught in the hospital, the cross-cradle hold, may actually be contributing to your nipple pain.
I know. That contradicts everything you have heard. The cross-cradle is practically gospel in maternity wards. Yet research tells a more complicated story: a 2016 Australian study of 653 mother-baby pairs found that this same technique worsened the incidence of nipple pain fourfold. Let that sink in. The “gold standard” hold may be the very thing keeping you in pain.
The best breastfeeding positions for newborns are the laid-back position, also called biological nurturing, the cross-cradle hold, and the football hold. Each supports deep latch, milk transfer, and maternal comfort. The right position depends on your birth type, breast size, baby’s latch strength, and your recovery needs.
Here is exactly what you will get in this article:
- Six evidence-based positions explained step by step, with “do this, not that” guidance
- A comparison table to find your ideal starting position in 60 seconds
- A latch confirmation checklist you can use mid-feed, right now
- Position guidance by birth type (C-section, vaginal, NICU)
- The real reason position affects milk supply (it is not what you think)
What Breastfeeding Positions for Newborns Really Mean
It Is Not About the Hold. It Is About the Dyad.
A breastfeeding position is not just a way to hold a baby. It is the entire biomechanical arrangement of two bodies, yours and your baby’s, that determines whether gravity assists or fights milk flow, whether your baby’s tongue can execute its natural wave motion, whether your spine is under strain or supported, and whether your infant’s primitive feeding reflexes are activated or inhibited.
Table of Contents
Positioning describes how you sit or lie and how you support your baby as they take the breast. Even small adjustments can make a big difference to how well your baby can breastfeed. Attachment, by contrast, describes the way the baby actually latches onto the breast. These two concepts are distinct but inseparable: position sets the stage for attachment. If the stage is wrong, the latch rarely recovers.
Evidence suggests humans evolved to breastfeed in laid-back positions, with babies upright against the chest. That means our default cultural assumption, sit up straight and hold the baby horizontally, may actually work against millions of years of mammalian design. This approach, sometimes called biological nurturing, is not a trendy alternative. It may be the original blueprint.
The Science of Position and Milk Transfer
Let me explain what happens during a deep latch in plain language, because once you understand this, everything else clicks.
As your baby nurses, a muscular wave starts at the tip of their tongue and moves backward. This rhythmical rolling action of the tongue and jaw massages your breast, squeezing the milk that lies in tiny pools beneath the areola into the nipple. To be effective, your baby needs to take more than the nipple into their mouth. They need to get far enough onto the breast so that the lower jaw and tongue can massage the pools of milk in the lower areola.
If your baby is only latched onto the nipple tip, they are basically sucking on a straw that is pinched shut. No amount of effort will extract the milk efficiently. Worse yet, the tongue and jaw rub the nipple itself instead of massaging the breast, and that is exactly what creates the cracking and bleeding that makes you dread every feeding session.
Position determines whether your baby can physically reach that deep tissue. A shallow position guarantees a shallow latch. A supported, aligned position opens the door to the kind of latch that drains the breast fully, protects your nipple, and signals your body to keep producing.
Position is not decoration. It is the mechanical foundation of every successful feed.
6 Breastfeeding Positions for Newborns: Step-by-Step Guide
There are many breastfeeding positions. Some may be more helpful than others in the early stages, when you and your baby are learning to breastfeed. This guide prioritizes the six most effective for the newborn stage, ordered from easiest to most situational.
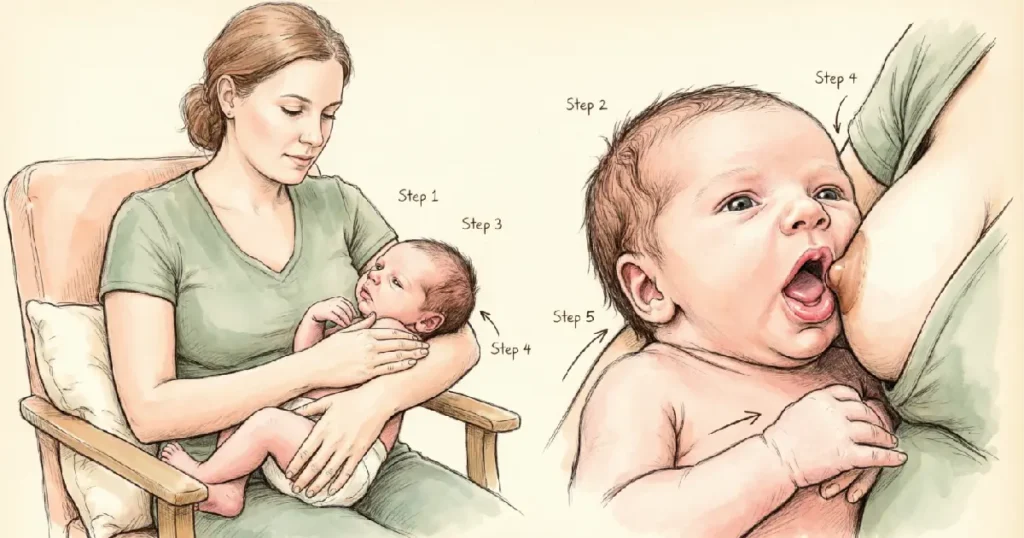
Position 1: Laid-Back, also called Biological Nurturing (Best Starting Position)
Step 1: Recline to about a 45-degree angle. Not flat. Use pillows to support your back, neck, and arms. You want to feel like you are settled in for a movie marathon, not a sit-up contest.
Step 2: Place your baby tummy-down on your chest, their entire front against your front. Chin, tummy, and legs all in contact. The whole front of the baby’s body should have full contact with the front of your body.
Step 3: Let gravity do the holding. The laid-back breastfeeding position uses gravity to hold your baby close, mold their body to yours, and allow them to feel safe and secure.
Step 4: Let your baby find the nipple using their natural rooting reflex. Do not force the latch. Babies can use gravity to latch onto the nipple without help. Your job is to create the conditions. Their job is to do the rest.
Step 5: Confirm the latch using the checklist below.
Do This: Allow your baby to self-attach with gentle guidance. Keep your hands relaxed on their back, not their head.
Not That: Do not force or push your baby’s head onto the breast. That triggers a defensive pull-back reflex and teaches your baby that the breast is a battle zone.
This position works with your baby’s natural instincts. It is calming for both of you, great for skin-to-skin contact, and particularly helpful if you have an overactive let-down reflex or excessive milk supply. Also ideal for sleepy newborns, large breast anatomy, forceful let-down, and the first days postpartum.
Nancy Mohrbacher, IBCLC, FILCA, puts it this way: “These laid-back positions not only make breastfeeding less work for mothers, they also make it easier for babies to take the breast deeply, especially during the early weeks.” This matters because deep latch during the early days is what prevents the nipple trauma cascade before it starts.
Position 2: Cross-Cradle Hold (Best for Latch Control)
Step 1: Sit upright in a chair with armrests. Place a pillow on your lap. Have water within reach. You will be here a while.
Step 2: Bring your baby across the front of your body, tummy to tummy. Hold with the arm that is not on the same side as the breast you are feeding from: left arm for right breast, right arm for left breast.
Step 3: Support the back of your baby’s head with your open hand. With your other hand, support your breast from the underside using a U-shaped hold, thumb on one side, fingers on the other.
Step 4: Guide your baby’s mouth to the breast. Aim their nose toward the nipple, then scoop the lower breast into a wide-open mouth. This is called the asymmetric latch technique, and it is the difference between a shallow, painful grip and a deep, effective one.
Step 5: Do not bend over or lean forward. Cradle your baby close to your breast instead.
Do This: Bring baby to breast. Never lean your breast down to the baby.
Not That: Do not grip the back of your baby’s skull. Support the neck and shoulders to allow natural head tilt. A clamped head equals a clamped jaw.
Important nuance: Although the cross-cradle is widely taught in hospitals, some research links it to increased nipple pain. A 2016 Australian study found the cross-cradle technique worsened nipple pain fourfold when compared to other approaches. If you experience consistent pain in this hold, transition to the laid-back or football hold and consult a lactation consultant. This position gives you maximum latch control, which is valuable, but that control should never come at the cost of your comfort.
Best for early breastfeeding days, latch difficulties, small babies, and the learning stage.
Position 3: Football or Clutch Hold (Best After C-Section or for Large Breasts)
Step 1: Sit on a bed or sofa with a firm pillow at your side. You want your baby supported at breast height without your arms doing all the work.
Step 2: Tuck your baby under your arm, lying along the side you are feeding on. Use pillows to support the baby and your arms. Your baby’s head is in your hand on the same side as the breast being used, upper body supported by your forearm.
Step 3: With that hand, control your baby’s head to bring the mouth in quickly for a good latch. Use your other hand to reach across and support and narrow your breast.
Step 4: Ensure your baby’s feet are tucked and supported, not dangling. Dangling feet create an unstable base, and an unstable baby breaks the latch repeatedly.
Step 5: Confirm deep latch using the checklist.
Do This: Keep your baby’s body parallel to the floor, tucked, horizontal, and fully supported.
Not That: Do not let your baby’s feet push against the back of the chair. That causes arching and latch breaking.
This position is great for newborns, especially small or premature babies, and for mothers recovering from a C-section. A 2021 study published in Breastfeeding Medicine found that the football hold was associated with significantly less incisional pain after cesarean section compared to the cradle hold. It offers excellent visibility of the latch and keeps pressure entirely off the abdomen.
Position 4: Cradle Hold (Best Once Latch Is Established)
Step 1: The cradle hold works best in a chair with armrests. Hold your baby in the arm on the same side as the breast you are feeding from, resting their head comfortably in the bend of your elbow, facing your breast.
Step 2: Place your arm on the chair’s armrest and use a pillow on your lap to lift your baby so you do not need to bend forward.
Step 3: With the arm not holding the baby, support your breast from the underside in a U-shaped or C-shaped hold.
Step 4: Ensure your baby’s head aligns with their body. No head turned to the side. A twisted neck makes swallowing harder.
Step 5: If using a breastfeeding pillow, make sure it does not lift your baby too high. Breasts should remain at their natural resting height to avoid sore nipples and a strained latch.
Do This: Let your baby’s ear, shoulder, and hip form a straight line.
Not That: Do not start here in the first one to two weeks. The cradle hold offers less head control than cross-cradle or football, and during the learning phase, that control matters.
Best for established feeders at two weeks and beyond, any breast size, and general daily use.
Position 5: Side-Lying (Best for Night Feeds and C-Section Recovery)

Step 1: Lie on your side with pillows to support your back and head. A pillow between your knees helps keep your hips aligned.
Step 2: Face your baby toward your breast, supporting them with one hand. With the other hand, grasp your breast and touch your nipple to your baby’s lips.
Step 3: Once your baby latches, use one arm to support your head and the other to help support and bring your baby close.
Step 4: Ensure your baby’s spine is straight, not twisted. Place a rolled blanket behind your baby’s back for added support.
Step 5: Safety note. After feeding in this position, always return your infant to a firm, separate sleep space alone, with no loose items, on their back.
Do This: Use a body pillow or rolled towel behind your own back for lumbar support. Your comfort matters too.
Not That: Do not attempt this position in the first week if you are still learning the latch. This position makes it harder to see how well your baby is latched, so it may be best once both you and your baby are used to breastfeeding.
Best for night feeds, C-section recovery, postpartum fatigue, and the second and third weeks onward.
Position 6: Koala, also called Upright Hold (Best for Reflux, Ear Infections, and Tongue-Tie)
Step 1: In the upright or koala hold, your baby sits straddling your thigh or on your hip, with their spine and head upright as they feed.
Step 2: Support your baby’s head and spine with one hand. Use the other for breast support.
Step 3: Ensure your baby’s chin is touching the breast, mouth is wide, lower lip is flanged out.
Step 4: Allow your baby’s knees to flex outward in a natural frog position for comfort.
Do This: Keep your baby’s ear, shoulder, and hip in vertical alignment.
Not That: Do not attempt without head support in early weeks. You can do this hold with a newborn if you give plenty of support, but it requires more active stabilization than other positions.
Best for babies who suffer from reflux or ear infections, who prefer to be upright, and for babies with tongue-tie or low muscle tone.
Position Comparison Table
| Position | Best For | Latch Control | Maternal Comfort | Birth Type | Difficulty |
|---|---|---|---|---|---|
| Laid-Back | First days, strong let-down, sleepy baby | Moderate | Very High | All types | Beginner |
| Cross-Cradle | Latch learning, small babies | Very High | Moderate | All types | Beginner |
| Football Hold | C-section, large breasts, premature baby | Very High | High | Ideal for C-section | Beginner |
| Cradle Hold | Established feeders (2+ weeks) | Moderate | High | Vaginal preferred | Beginner |
| Side-Lying | Night feeds, recovery, fatigue | Moderate | Very High | C-section and vaginal | Intermediate |
| Koala (Upright) | Reflux, ear infections, tongue-tie | High | High | All types | Intermediate |
The Latch Confirmation Checklist
You have a good latch when: the experience is comfortable with no pain, more areola is visible above your baby’s mouth than below, their mouth is wide open, their lower lip is turned out, and their chin is touching, or nearly touching, your breast.
- You can hear swallowing sounds, not just sucking
- Your baby’s cheeks are full and rounded, not hollowed
- Your nipple is round, not lipstick-shaped, after feeding
- The latch feels like a pulling sensation, not pinching or burning
- Your baby’s ears wiggle slightly during active feeding
Meet Sarah: From Cracked Nipples to Confident Nursing

Sarah, a 25-year-old first-time mother from Ohio, was eight days postpartum after a planned C-section. She was exclusively using the cross-cradle hold, the position the hospital lactation team had demonstrated during her stay. She had practiced it diligently. She assumed the pain was just part of the process.
By day five, she had cracked, bleeding nipples and a baby who screamed at every feeding attempt. She would cry before each session, bracing herself. Her lactation consultant used the LATCH scoring system, a standardized tool that assesses how well a baby latches and transfers milk. The score confirmed what Sarah already suspected: her baby was extracting very little milk, and the positioning was causing a shallow, nipple-only latch.
The consultant suggested one change: switch to the football hold. Because Sarah had a C-section incision, the football hold eliminated all pressure on her abdomen. More importantly, it gave Sarah full visibility of her baby’s mouth. For the first time, she could see that her baby was only grasping the nipple tip. She learned to aim her baby’s nose toward the nipple and guide a wide-open, asymmetric latch.
Within 48 hours of the position switch, Sarah’s nipple pain dropped dramatically. By week three, she had introduced the laid-back position for nighttime feeds, and she breastfed successfully for 11 months.
Sarah’s solution was specific to her situation. Yours will be too. The point is not to copy her path. The point is to know that there is a path, and the right position, your position, is waiting for you to find it.
Finding Your Position: A Decision Framework
Breastfeeding Position by Situation: Why Context Beats Convention
The best position is any position that ensures your baby is transferring milk and does not cause you pain. Many times, it is simply a matter of personal preference. Some positions feel more comfortable for some women than others. But context dramatically narrows the choice. Start here, with these three questions.
Question 1: What type of birth did you have?
If you had a vaginal delivery, start with laid-back or cross-cradle. Your body has a full range of motion, and both positions give you excellent control during the learning curve.
If you had a C-section, start with the football hold. After a cesarean, reclining with your baby across your shoulder or tucked under your arm allows nursing without weight or pressure on your wound. The side-lying position is also excellent once you are comfortable with the latch.
Question 2: Does your baby have any special needs?
For reflux, tongue-tie, or ear infections, use the koala upright hold. Gravity becomes your ally, and the vertical position reduces discomfort for your baby.
For a premature baby or one with low muscle tone, use the football hold with Dancer Hand support. This gives you maximum control over head positioning.
For a sleepy or low-interest newborn, laid-back breastfeeding with skin-to-skin contact can maximize your baby’s natural instinct to breastfeed.
Question 3: Are you experiencing specific physical issues?
For sore nipples, switch away from cross-cradle. Try football or laid-back. A 2021 meta-analysis published in BMC Pregnancy and Childbirth found that the laid-back position was proven to decrease the incidence of nipple pain and nipple trauma and was conducive to achieving correct latching position.
For a strong let-down or oversupply, the laid-back position helps those who produce more milk than their babies drink or whose milk releases quickly. Gravity works against the flow, giving your baby more control.
For back pain, do a position audit. Bring your baby to you, not you to the baby. Bending over your baby can lead to back and neck problems that compound over weeks and months of feeding.
Practical Resources
- A nursing pillow. Having pillows handy helps take the strain off your back, shoulders, and wrists.
- A consultation with a certified IBCLC for in-person positioning assessment.
- A position rotation schedule. Switching infant breastfeeding positions throughout the day may help empty the breasts more fully and reduce the risk of clogged ducts or mastitis.
- The La Leche League International Helpline for free peer support from trained breastfeeding advocates.
- A mirror or smartphone camera to observe your latch in real time before a consultant visit.
Common Mistakes and How to Avoid Them

Mistake 1: Leaning Your Breast Down to the Baby
This is the single most common positioning error I see. Every exhausted new mother does it instinctively. You cup your breast and lean forward, bringing it to your baby’s mouth instead of bringing your baby to the breast.
Here is the fix: before you even attempt to latch, check your posture. Your shoulders should be relaxed, dropped away from your ears. Your back should be supported. Your baby should be lifted to nipple height by pillows or your arm. If you feel yourself bending forward, stop, reset, and lift your baby. This alone can resolve neck and shoulder pain that has been building for days.
Mistake 2: Using Only One Position Exclusively
When you find something that works, the temptation is to lock it in and never deviate. I understand the impulse. But using a single position at every feed means the same milk ducts get drained the same way every time, while others may never fully empty.
The solution is simple: rotate at least two positions across your feeding day. A 2021 study in Breastfeeding Medicine comparing positions after C-section demonstrated that both cradle and football holds had distinct advantages, and prenatal training should cover all breastfeeding positions because no single position serves every situation. Even alternating between just two positions can reduce your risk of clogged ducts and mastitis.
Mistake 3: Chasing the “Perfect” Latch Obsessively
Some mothers get so fixated on achieving the textbook latch, lips flanged, mouth wide, areola invisible, that they break and re-latch their baby a dozen times per session. This frustrates your baby, damages your nipple through repeated friction, and creates a stressful environment around feeding.
If the latch is pain-free and your baby is swallowing rhythmically, it is likely adequate, even if it does not look exactly like the diagram. Signs of a good latch according to the Office on Women’s Health include comfort without pain or pinching, your baby’s chest resting against your body, and little or no areola visible depending on your anatomy. Perfection is not the goal. Pain-free, effective milk transfer is the goal.
Mistake 4: Ignoring Your Own Body Mechanics While Fixated on the Baby
Competitors tell you endlessly how to hold your baby. Almost no one tells you how to hold yourself. Yet breastfeeding-related neck pain is prevalent in nursing mothers, and the biomechanical considerations of ergonomically safe positions have been understudied until recently.
Fix this by doing a pre-feed body scan. Are your feet flat on the floor? Are your shoulders relaxed? Is your lower back supported? Is your wrist straight, not bent sharply? These things matter after the third, fourth, and fifth feed of the day. Your body is the foundation of every feed. If your foundation is compromised, nothing above it works well.
Frequently Asked Questions
What is the best breastfeeding position for a newborn with a bad latch?
The cross-cradle and football hold offer the most head control for correcting a bad latch. The football hold gives you a clear, unobstructed view of your baby’s mouth, making it easier to see whether they are grasping deeply or just the nipple tip. If pain persists, try the laid-back position, which activates your baby’s natural rooting reflex and requires less active repositioning from you. Always consult an IBCLC if latch pain continues beyond one week.
What breastfeeding positions work best after a C-section?
After a C-section, the football hold and side-lying position are typically most comfortable because they keep pressure entirely off your abdominal incision. The side-lying position is helpful for C-section recovery because it allows you to lie down while feeding. The laid-back position is also gentle on your abdomen, especially when your baby lies vertically or diagonally rather than across the incision. Avoid the cradle hold in the first one to two weeks, as baby weight resting on your lap may strain your incision site.
How do I know if my baby is in the right breastfeeding position?
Your baby is in the right position when their body forms a straight line, ear, shoulder, and hip aligned, tummy facing your tummy, mouth wide open with the lower lip flanged out, and chin touching your breast. You should feel pulling but not pain and hear rhythmic swallowing. If your nipple exits the feed shaped like a lipstick, the latch was shallow. A correctly positioned baby does not need to turn their head to drink, and their cheeks remain full and rounded throughout the feed.
Can breastfeeding position affect milk supply?
Yes, significantly. Comfortable positioning and a deep latch are important for establishing and maintaining milk production. A shallow latch from poor positioning means less milk is extracted per feed, signaling your body to produce less over time. Additionally, using only one position can lead to incomplete breast drainage, increasing clogged duct and mastitis risk. Rotating positions helps ensure full, even breast emptying and optimal supply signals across all milk ducts.
What is the laid-back breastfeeding position and why is it recommended?
The laid-back position, also called biological nurturing, involves reclining at a 45-degree angle with your baby lying tummy-down on your chest. It works with your baby’s natural instincts, is calming for both of you, supports skin-to-skin contact, and helps newborns latch using primitive feeding reflexes like rooting and suckling. Evidence suggests humans evolved to breastfeed this way. It is especially helpful for strong let-down, oversupply, and sleepy or uninterested newborns who need gentle encouragement to engage.
Is it okay to use different breastfeeding positions at different feeds?
Absolutely. In fact, it is encouraged. There are many ways to position yourself while breastfeeding. What is most important is what works for you, so try all positions until you and your baby are comfortable. You may even use different positions for each feeding. Rotating positions also helps prevent clogged milk ducts by ensuring different milk ducts are drained at different angles throughout the day, which is one of the most effective, non-pharmaceutical strategies for preventing mastitis.
Final Takeaway
Here is the truth that most breastfeeding guides are too polite to say: the position that works best is not necessarily the one your nurse taught you, the one your mother-in-law swears by, or the one that looks prettiest in the Instagram photo. It is the position that lets your baby transfer milk effectively while you remain pain-free. Period.
If that is the football hold at 9 AM and side-lying at 2 AM, great. If you never use the cross-cradle again after reading this, also great. Your body, your baby, your rules. The research is clear. Multiple positions reduce nipple trauma, improve breast drainage, and give you options when one approach stops working. You do not need to master all six positions today. You need one that works right now. Start there. Let the rest come with time.
My Closing Remarks
I have watched mothers sob in lactation consultations, convinced their bodies were broken, when the only thing broken was the advice they had been given. Positioning is not a minor detail. It is the difference between a breastfeeding journey that ends in trauma after two weeks and one that stretches into months of confident, connected feeding. If you take nothing else from this article, take this: pain is information, not a requirement. Your baby needs a mother who is not dreading every feed far more than they need any specific hold. Trust your body enough to try something different tonight.




